Rare Diseases: Opportunity for SC to Enable Access to Medicines

Two recent interim orders of the Supreme Court have pushed the lives of people living with rare diseases to the edge. These two orders were passed in two separate special leave petitions (‘SLP’) filed by the Union challenging the High Court orders of Delhi and Kerala which advanced access to treatment for rare diseases. These interim orders virtually blocked any possibility of affordable treatment to many people living with rare disease (‘PLRD’) who need treatments that are available at a high cost such as Spinal Muscular Atrophy (‘SMA’), Cystic fibrosis (‘CF’), Duchenne muscular dystrophy (‘DMD’) etc. Apart from staying the orders of the High Courts, these interim stay orders raise concerns about the scope of the right to life guaranteed under Article 21 of the Constitution. In a letter, nearly 220 mothers and caregivers of children living with SMA and CF have written to the Chief Justice of India (‘CJI’) seeking justice.
The letter requests CJI “to take “suo motu” cognizance of this dire situation and direct the expeditious resolution of pending legal cases concerning rare disease treatments. We further urge the judiciary to reinforce the government’s obligation to ensure access to life-saving medicines through compulsory licensing, price control, and local production to allow price-lowering generic competition, as provided under Indian law”.
Instead of taking law and policy measures to bring down the cost of medicines through local production under the existing law and policy framework, the Union is citing the exorbitant cost of treatment as a reason for not providing assistance beyond the one-time assistance of Rs 50 lakhs to each PLRD.
Further, the letter also seeks answers to the following questions.
-
“Why are our children dying when India has the capability to produce these life-saving medicines at a fraction of the cost?
-
Why do courts prioritize patent enforcement over the fundamental right to life under Article 21 of the Constitution?
-
Why do our legal cases remain indefinitely stalled while our children's lives are slipping away?”
These litigations and the letter challenge the lack of effective implementation of the National Policy for Rare Diseases 2021 (NPRD). The failure of the effective implementation of NPRD primarily emanates from the failure of the Union government to take measures to facilitate the availability of medicine/treatment for rare diseases. Instead of taking law and policy measures to bring down the cost of medicines through local production under the existing law and policy framework, the Union is citing the exorbitant cost of treatment as a reason for not providing assistance beyond the one-time assistance of Rs 50 lakhs to each PLRD. In the absence of availability at an affordable price, neither individuals nor state governments can procure medicine on a sustainable basis resulting in the denial of the right to life and health. Often the high prices result in the denial of access and thus violate the enjoyment of the right to health.
Further, there is no transparency with regard to the amount distributed under the Rs 50 lakh assistance.
The National Policy for Rare Diseases
The NPRD came into effect in 2021, and “…aims at lowering the incidence and prevalence of rare diseases based on an integrated and comprehensive preventive strategy encompassing awareness generation, premarital, post-marital, pre-conception and post-conception screening and counselling programmes to prevent births of children with rare diseases, and within the constraints on resources and competing health care priorities, enable access to affordable health care to patients of rare diseases which are amenable to one-time treatment or relatively low cost therapy.” NPRD divides rare diseases into the following three categories to provide treatments:
-
Disorders amenable to one-time curative treatment
-
Diseases requiring long-term/lifelong treatment having relatively lower costs of treatment where annual or more frequent surveillance is required.
-
Diseases with definitive treatment but having very high cost and lifelong therapy
The policy implementation strategy of NPRD envisages the role of state governments only with regard to the second category. It states: "State Governments can consider supporting patients of such rare diseases that can be managed with special diets or hormonal supplements or other relatively low-cost interventions (Diseases listed under Group 2).” Thus, the Union shoulders the responsibility of facilitating the treatment for rare diseases falling under categories 1 and 3. The policy also provides for a one-time assistance of Rs 50 lakhs for the treatment, which will be provided through the twelve Centres of Excellence (‘CoE’) designated to implement NPRD. However, the implementation of the policy so far is not up to the desired level and a large number of PLRD are not able to access treatment.
Though the one-time assistance of Rs 50 lakhs sounds like a huge amount, it is not enough to support even one year of treatment due to the exorbitant prices of medicines/treatment of rare diseases belonging to category 3. As a result, people living with SMA, CF or DMD are not in a position to benefit from the assistance.
For instance, only an eight to nine month supply of Redisplam can be supported with Rs 50 lakhs even if the government procures each bottle at Rs 2,20,000 i.e., after a heavy discount from the maximum retail price ofRs 6,20,000 per bottle. Similarly, the price of Trikafta for the treatment of CF costs USD 320,000 per year. To support beyond Rs 50 lakhs, NPRD established a crowd funding platform. Since its establishment, nearly 3209 patients registered on the platform were able to raise only Rs 3,72,285.
Further, there is no transparency with regard to the amount distributed under the Rs 50 lakh assistance. In response to a question in Rajya Saba, the Ministry of Health informed that 1000 patients received financial assistance through the 12 CoEss. However, the allotted financial resources show these 1000 patients might not have received Rs 50 lakhs each because the allocated financial resources during the last three financial years amounted only to Rs 191.87 crores (Rs. 35 crores for FY 2022-23, Rs. 74 crores for FY 2023-24 and Rs. 82.87 crores for FY 2024-2). However, the Ministry of Health did not provide any information on actual spending as well as details like the name of diseases, number of patents and corresponding CoE through which the assistance was provided despite being asked. However, the response to another parliament question in February 2024 shows that only 48.7 p of around ₹109 crores disbursed by the Ministry in the last three years was utilised.
To address the affordability of the medicines, NPRD contains the following four measures.
-
Research and development of new drugs as well as repurposing of existing drugs in cooperation with the Indian Council of Medical Research (‘ICMR’), Department of Biotechnology, Department of Pharmaceuticals, Department of Science and Technology and Council of Scientific & Industrial Research
-
Reduction in custom duties on import of medicines related to rare diseases
-
Document and make publicly available the prices of drugs for rare diseases and work towards affordability of drugs for rare diseases
-
Measures for creating a conducive environment for indigenous manufacturing of drugs
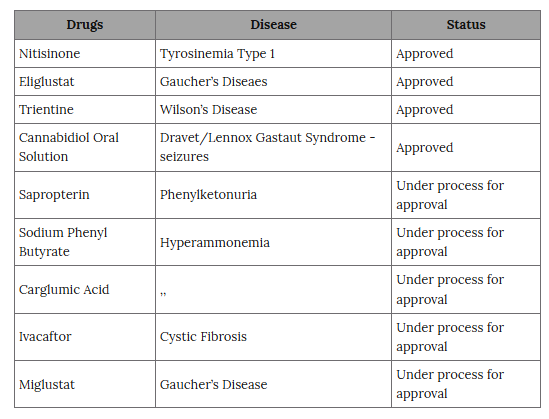
Generally speaking, apart from protein supplements there are two types of medicines available for the treatment of rare diseases - small molecules and cell and gene therapy. Considering Indian pharmaceutical capabilities in the small-scale molecules there are no technological barriers for the low-cost local production of this class of medicines. There are effective small molecules for the treatment of rare diseases along with cell and gene therapy. Cost-effective local production of cell and gene therapy (biologics) is resource and time-intensive as compared to the small molecules. To date, R&D initiatives have been undertaken to develop nine medicines for seven diseases and out of these nine medicines four are already approved for marketing and five are under development. However, these initiatives do not cover small molecules currently under patent protection.
NPRD recognises the importance of local production of medicines and diagnostics for rare diseases to facilitate sustainable and affordable availability of medicines. The generic introduction through local production can reduce the price of patented medicines drastically often to below 95 percent. For instance, recently pharmaceutical firm Natco announced the price of a generic version of Risdiplam for one bottle at Rs 15,900 against Roche’s price of Rs 6,20,000. However, the generic version can come into market only after the verdict of the Court on an ongoing patent infringement dispute. It also implicitly reconciles the patent barrier for the local production of generic versions of medicines and diagnostics because product patent prevents the local manufacturers from producing the generic version during the patent protection period.
In this regard, Para XI of the implementation strategy of NPRD states: “Department of Pharmaceuticals, Department for Promotion of Industry andInternal Trade (DPIIT) will be requested to promote local development and manufacture of drugs for rare diseases by public and private sector pharmaceutical companies at affordable prices and take legal/legislative measures for creating a conducive environment for indigenous manufacturing of drugs for rare diseases at affordable prices. PSUs could also be encouraged for local manufacturing of drugs for rare diseases”. However, no measure taken to implement this paragraph especially related to facilitating the local production of patented medicines is in the public domain.
Table: Local Production Initiatives for Rare Diseases
Litigations
The lack of access to expensive medicines including those mentioned in Table 1 resulted in litigations in various High Courts and the Supreme Court. These litigations deal with various aspects of access to affordable treatment covering access to both cell and gene therapy and small molecules. In the April 8 order, the Supreme Court relisted 5 SLPs before the Bench presided over by Justice P.S. Narasimha. The hearing is expected to provide justice to thousands of PLRDs and their families.
Union of India v Master Arnesh Shaw: The Government of India filed this SLP to challenge the order of the Delhi High Court to facilitate treatment to PLRDs. On October 4, 2024, the Delhi High Court issued an order which contains a set of instructions to various entities including the Union government and companies. This petition was initially seeking financial assistance for gene therapy for DMD. However other PLRDs also joined the petition seeking the government's intervention including in financial aid for the treatment of SMA, Goucher diseases etc. One of the important directions to the Union government is to establish a fund for providing the treatment of PLRDs. It states:
“The Union of India shall establish the National Fund for Rare.Diseases (‘NFRD’) for which a sum of Rs. 974 crores, as per the recommendation of the NRDC, and pending approval of the MoHFW, shall be allocated for the financial years 2024-25, 2025-26. Similarly, the same amount if not a higher amount, shall be allocated for the next two financial years of 2026-27 and 2027-28.”
Courts also directed pharmaceutical companies to supply medicines/therapies at an agreed price with National Research Development Corporation (‘NRDC’). The order states:
“In the case of rare diseases, if therapies and medicines are not available, the Government is also empowered under the Patents Act, 1970 to use the invention under Section 100 of the Patents Act, 1970 for Government use, and permit manufacturing by a third party subject to payment of royalty to the patentee”.
However, there is no direction to consider the use of Section 100. The Supreme Court granted an interim stay on the order hence the implementation of the directions is in limbo.
Unfortunately, while granting the interim stay orders the Supreme Court did not take into account the larger questions of right to life and health.
Union of India v. Seba P.A.: This SLP is against the order of a Division Bench of the Kerala High Court, which refused to stay the order of a Single Bench to continue the treatment beyond Rs 50 lakhs assistance under NPRD. Seba, a person living with SMA, approached the High Court seeking direction from the court regarding the invocation of Section 100 of the Patents Act to facilitate the availability of affordable access to Risdiplam. According to the petitioner, the patent protection on Risdiplam not only resulted in exorbitant pricing but also prevented the possibility of affordable generic production of Risdiplam in India. The exorbitant price is affecting the enjoyment of the right to life and health under Article 21. Therefore, the petitioner submitted that the use of Section 100 is important to protect the right to life and health. The petitioner also got an interim remedy to obtain Risdiplam under NPRD assistance. The interim stay order resulted in the disruption of the treatment to the petitioner, which was restarted after Roche agreed to provide treatment for a year.
Unfortunately, while granting the interim stay orders the Supreme Court did not take into account the larger questions of right to life and health. Further, it subscribes to the argument of the Union government without looking into the possibilities of existing law and policy measures to reduce the price of these medicines. Instead, the Court subscribed to the resource constraint arguments of the Union government. There are public interest safeguards in the Patents Act to enable the availability of generic versions of many rare disease medicines especially those mentioned in Table 1 at an affordable price.
Indian Patents Act and public interest safeguards
The Patents Act contains various public interest safeguards to facilitate affordable access to patented medicines. These safeguards are :
-
Section 47 allows the importation of medicine by the government or on behalf of the government for the purpose merely of its own use or for distribution in any dispensary, hospital or other medical institution maintained by or on behalf of the Government.
-
Section 66 the Central government is empowered to revoke the patent when “a patent or the mode in which it is exercised is mischievous to the State or generally prejudicial to the public,”
-
Section 84 allows the issuance of the compulsory license when : (a) the reasonable requirements of the public with respect to the patented invention have not been satisfied, or (b) the patented invention is not available to the public at a reasonably affordable price, or(c) that the patented invention is not worked in the territory of India.
-
Section 100 permits the government use of an invention for any authorised person by the government after paying a reasonable royalty.
-
Section 102 grants the power to the Union government to acquire the patent after paying compensation.
While these public interest safeguards in the Patents Act are important in facilitating the availability of affordable generic versions, it does not offer any role to patients, the most affected parties, in the invocation of these safeguards. As a result, PLRDs are at the mercy of the pharmaceutical companies or the government for the use of these safeguards. In other words, the Patents Act does not contain any provision which allows PLRDs to initiate the process for the invocation of these public interest safeguards. One possible option is to approach the courts through the writ petition. However, the effectiveness of this route is to be determined in the coming days. Towards this end, courts are to carry out the hearing on the merits of petitions such as the Seba P.A. litigation seeking invocation of Section 100 to facilitate the generic production of Risdiplam or X v. Union of India (in the Bangalore Bench of the Karnataka High Court) seeking direction for the government use for the generic production of Trikafta.
The willingness of the Supreme Court to grant interim stay orders without looking into the details of law and policy measures that can be taken to facilitate affordable access to treatment, raises not only moral and ethical questions but also disrupts the ongoing treatment of many PLRDs, which raises serious concerns on the enjoyment of the right to life and health. The Union government has not informed the Court of the steps which can be taken to facilitate the generic version of patented protected medicines to facilitate affordable access. The Union seems to impose a unilateral moratorium on the use of public health safeguards like compulsory licenses to facilitate access. According to news reports which were later denied, the government assured US multinationals not to issue any compulsory licenses and even took a stand against the use of compulsory licenses during the second wave of COVID 19 in 2021.
The remarks of the CJI on the international ramifications of compulsory licenses also show that such skewed views on such effective public interest safeguards prevail even among the judiciary.
This view totally ignores the legislative intent behind these public interest safeguards and holds the view that the government holds the discretion in invoking these safeguards. The remarks of the CJI on the international ramifications of compulsory licenses also show that such skewed views on such effective public interest safeguards prevail even among the judiciary.
However, these views not only overlook the statutory provisions but also fail to answer the question as to how much discretion is available to the government when fundamental rights are being violated. The new bench is expected to provide clarity on these issues.
K. M Gopakumar is a Senior Researcher and Legal Advisor at Third World Network (TWN) and based in New Delhi, India.
Courtesy: The Leaflet
Get the latest reports & analysis with people's perspective on Protests, movements & deep analytical videos, discussions of the current affairs in your Telegram app. Subscribe to NewsClick's Telegram channel & get Real-Time updates on stories, as they get published on our website.